
Episode 240: Cannabis and Psychosis: The Link Between THC Use and Mental Health Risks
Daniel Cuevas, Liam Browning, MD; Christopher Campbell, Danielle Liu, David Puder, MD
Corresponding Author: David Puder, MD
Reviewer: Erica Vega, Joanie Burns, PMHNP-BC
By listening to this episode, you can earn 1.25 Psychiatry CME Credits.
Other Places to listen: iTunes, Spotify
The authors declare no conflicts of interest and have no financial relationships with any pharmaceutical or cannabis companies.
We are at a time when cannabis use is increasing, becoming normalized as a healthier recreational option, and when higher-potency versions are increasingly accessible. The societal impact is still unfolding. Yet, as clinicians in the field, it is not uncommon to observe new cases of psychosis emerging in the wake of heavy, high-potency THC use, or existing patients with schizophrenia decompensating following new or increased consumption.
Real-world clinical scenarios underscore why this issue is so important. In one case, a young man with a long history of daily cannabis use began experimenting with “dabbing,” a method of inhaling extremely concentrated THC. Within weeks, he became intensely paranoid and hypervigilant—convinced that strangers in a black truck were following him—and grew too anxious to sleep at night. His downward spiral was halted only after he was hospitalized, treated with antipsychotic medication, and most importantly, stopped using cannabis. Once the high-THC dabs were out of his system, his paranoia and delusions quickly resolved.
In another case, a patient with an existing psychotic disorder remained trapped in persistent psychosis despite taking antipsychotic medication, simply because he continued to smoke marijuana daily. His family watched in frustration as each day of cannabis use sustained his hallucinations and erratic behavior. Only when they intervened—setting firm limits around car use (that enticed him to quit THC)—did his mind clear. In a matter of months, this individual experienced a remarkable turnaround to the point of successfully returning to college.
Cases like these have become increasingly familiar to psychiatrists and emergency physicians, reflecting a pattern seen in hospitals and clinics across the nation. They raise pressing clinical questions about the link between cannabis and psychosis. Can frequent use of high-potency THC actually trigger psychotic episodes or worsen an underlying mental illness? How does cannabis interact with the developing adolescent brain, and could early heavy use increase the risk of disorders like schizophrenia in vulnerable individuals? In the pages that follow, we will explore these questions in depth. We will examine the latest scientific research on cannabis’s impact on brain chemistry and neurodevelopment, review what is known about its role in psychotic illnesses, and discuss why today’s high-THC cannabis may pose unique challenges compared to the past.
Cannabis And Mental Health: Exploring The Connection Between Cannabis Use And Psychosis
The Growing Popularity of Cannabis and Its Mental Health Impacts
Cannabis is an increasingly popular recreational drug, with 50% of Americans reporting having smoked marijuana at least once in their lifetime as of 2023, compared with just 4% in 1969 (McCarthy, 2023). Moreover, there has been a 15-fold increase in daily cannabis users from 1992 to 2022 (Caulkins, 2024).
As of 2021, according to the Substance Abuse and Mental Health Services Administration (SAMHSA, 2022b), up to 19% of Americans (approximately 52.5 million individuals) admitted to using marijuana at least once in the last year. Notably, in young adults (ages 18 to 25), use in 2021 was as high as 35.4%, followed by 17.2% of adults aged 26 and older, and 10.5% of adolescents aged 12 to 17 (SAMHSA, 2022b).
When examining daily cannabis use (defined as using cannabis at least 20 times in the last 30 days), 10.4% of young adults ages 19-30 engage in daily use, followed by 7.5% of adults ages 35 to 50, followed by 5.2% for adults ages 55-65 (Patrick et al., 2024). For comparison, the total population of daily marijuana users has now surpassed that of daily alcohol users (17.7 vs 14.7 million, respectively). Furthermore, the median alcohol consumer reports alcohol use 4 to 5 days per month, whereas the median cannabis user engages in cannabis use 15 to 16 days per month, highlighting the significant differences in typical use patterns between these commonly used recreational substances (Caulkins, 2024). Additionally, a 2014 longitudinal study by Hughes et al. found that on average daily users will use marijuana 3.2 times per day, leading to a consistent intoxication during waking hours. Consistent with prior prospective studies, this study also demonstrated that social factors and availability were the two most powerful predictive factors of marijuana use.
This increase in cannabis use coincides with a significant shift in cannabis policies and an increase in accessibility of cannabis over the last decade. As of April 2025, there are only 4 states where cannabis is completely illegal; the other 46 states have various forms of legality including legal for medicinal purposes, legal for recreational use, decriminalized, or some combination of these factors (DISA, 2025). However, despite recreational cannabis remaining illegal in more than half of U.S. states, it is nevertheless widely available due to loopholes in the 2018 Agriculture Improvement Act (commonly known as the Farm Bill), which allows for the legal sale of chemically similar compounds, produced through minor molecular modifications, that nonetheless have the same psychoactive effects of cannabis.
Unfortunately, despite the widespread public perception of cannabis as a relatively benign substance, cannabis use continues to be associated with a wide array of significant and deleterious mental and physical health effects. In this episode on cannabis, we aim to provide an evidence-based exploration of cannabis use, covering its use patterns, pharmacology, mental and physical health effects, and societal implications. By the end, we hope to equip listeners with a comprehensive and scientifically grounded perspective regarding this increasingly utilized substance.
“Marijuana Use in the Past Year: Among People Aged 18 or Older; by State, Percentages, 2021”

Note. Reprinted from “2021 National Survey on Drug Use and Health: National maps of prevalence estimates, by state.”, by Substance Abuse and Mental Health Services Administration (SAMHSA)., 2022a, U.S. Department of Health and Human Services. Figure 2e..
The Rising Potency of Cannabis and Its Mental Health Implications
Not only has cannabis use increased, but the potency of the cannabis itself has increased as well. Average THC levels in cannabis were around 4% in the 1990s, whereas modern strains can exceed 17-28% (Backman, 2023; Stuyt, 2018).
THC Concentrates and Their Increasing Availability
Forms of cannabis with concentrations of THC exceeding 90%, also known as “THC concentrates,” are also becoming more commonplace, allowing for rapid consumption of high amounts of THC. Additionally, the availability and ease of use of THC vaporizers are points of concern, as people can use them without needing to prepare the substance for consumption, and they can be carried and used discreetly since they don’t require flower or produce the distinctive smell associated with flower. Moreover, high potency, bite-sized edibles make oral ingestion of high doses incredibly easy. Often, the delay in experiencing the effects of edibles, which can sometimes exceed two hours, can lead individuals to consume additional edibles at higher quantities than intended.
Understanding Cannabis And Its Effects On The Brain
The Endocannabinoid System: A Key Mechanism for THC’s Action in the Brain
Before describing how cannabis influences the brain and body, it is important to describe the body’s natural system it is acting on: the endocannabinoid system. The endocannabinoid system is a neuromodulatory network critical for maintaining homeostasis in many different domains through regulating appetite, sleep, memory, learning, emotional responses, movement, inflammation, and pain perception, to name a few (Lutz, 2020). Specifically, its primary mechanism in the central nervous system (CNS) is maintaining homeostasis of synapses via retrograde synaptic transmission. For example, if neuron A is exciting neuron B too much, neuron B can send endocannabinoids such as 2-arachidonoylglycerol (2-AG) back to neuron A. This will suppress neuron A’s activity and weaken the synapse between the two neurons.
The endocannabinoid system consists of cannabinoid receptors (i.e., CB1 and CB2), endogenous ligands (such as anandamide and 2-arachidonoylglycerol), and regulatory enzymes and transporters, which control synthesis and degradation of endocannabinoids (Hillard, 2015).
The Role of Cannabinoid Receptors in Mental Health
The two primary cannabinoid receptors are CB1 and CB2, both of which are G protein-coupled receptors (Lutz, 2020):
CB1 receptors (CB1Rs) are expressed throughout the central nervous system, on neurons, astrocytes, and microglia, but most densely on presynaptic neurons in brain regions such as the prefrontal cortex, hippocampus, anterior cingulate cortex, and cerebellum. They are particularly prevalent on GABAergic interneurons, where they regulate inhibitory neurotransmission, and to a lesser extent on cortical glutamatergic projection neurons. When CB1Rs are activated, they inhibit presynaptic voltage-gated calcium channels and increase potassium channel activity, leading to suppressed release of neurotransmitters and to decreased synaptic transmission. This retrograde signaling mechanism is central to the endocannabinoid system’s ability to maintain homeostasis through fine-tuning neural activity for synaptic plasticity, implicating it in learning, memory, and neurodevelopment.
CB2 receptors (CB2Rs), by contrast, are expressed mostly on immune cells of the periphery (lymphocytes, macrophages, etc.). However, CB2Rs are upregulated on immune cells of the brain (microglia and macrophages) in response to insults such as stroke, pain, and neuroinflammation.
THC and the Endocannabinoid System
Endocannabinoids, the system’s endogenous ligands, include anandamide (AEA) and 2-arachidonoylglycerol (2-AG), both derivatives of arachidonic acid. They are both synthesized on-demand and passively diffuse into the synapse, so they are not stored in vesicles.
Anandamide acts as a partial agonist at CB1Rs and TRPV1 (the capsaicin receptor, which responds to temperature) and is constantly released to provide steady modulation of synaptic activity, while 2-AG, a full agonist at both CB1 and CB2 receptors, is released retrogradely in response to heightened neural activity. Notably, endocannabinoids may also alter neurotransmission via other mechanisms, including interactions with neurosteroids (glucocorticoids, pregnenolone, etc.), mitochondria, and glial cells.
Endocannabinods play an important role in regulating mood and anxiety (Patel & Hillard, 2009), and are thought to increase with exercise and to play some role in producing the runner’s high (Siebers et al., 2021). Some early evidence suggests people with anxiety and PTSD may have lower levels of endocannabinoids (Bassir Nia et al., 2019), and phase 2 trials of CB1 antagonists were discontinued due to increased risk of suicide (Cohen et al., 2024), implicating them in psychiatric symptoms.
How THC and CBD Work in the Brain: Key Differences Explained
THC acts as a partial agonist at CB1Rs, thus mimicking anandamide. However, it does so with more persistent and indiscriminate binding across the brain, disrupting the balance of neuronal excitation/inhibition, and subsequently impacting cognition, mood, perception, and memory (Mayo et al., 2020). THC also induces euphoria by disinhibiting dopamine release in the reward system. Specifically, in the ventral tegmental area (VTA), THC inhibits GABAergic neurons that normally suppress dopamine activity, resulting in increased dopamine release in the nucleus accumbens and prefrontal cortex.
THC vs. CBD: Key Differences in How They Affect the Brain
Unlike THC, cannabidiol (CBD) does not produce psychoactive effects and interacts with the endocannabinoid system more indirectly. It does not significantly bind to CB1 or CB2 receptors, but instead inhibits fatty acid amide hydrolase (FAAH, the enzyme responsible for degrading anandamide) to prolong the effects of anandamide. Additionally, CBD interacts with serotonin 5-HT1A and TRPV1 receptors, and may also act as an orthosteric modulator of CB1R through reducing the binding of THC.
It is worth noting that the practice of breeding cannabis plants to maximize THC concentration leads to a decrease in CBD. CBD may counteract some of the anxiogenic effects of high doses of THC (Englund et al., 2013; Karniol et al., 1974; Zuardi et al., 1982; Solowij et al., 2019), although that point is still the subject of debate (Hindocha et al., 2015; Karschner et al., 2011; Arkell et al., 2021; Englund et al., 2023; Lawn et al., 2023).
Cannabinoid Pharmacology: The Absorption, Distribution, And Action Of THC And CBD
Absorption (Lucas et al., 2018)
Inhalation: When cannabis is smoked or vaporized, THC and CBD (as well as dozens of other phytocannabinoids, terpenoids, and flavonoids) are rapidly absorbed through the lungs, leading to quick onset of effects. This method bypasses first-pass metabolism. THC is highly lipophilic, meaning it can cross the blood-brain barrier quickly and exert psychoactive effects within minutes. Peak plasma concentrations of THC are typically achieved within 3–10 minutes (50-150 ng/mL via flower and up to 200-300 ng/mL with concentrate [vapes, resin, etc.]).
Oral Ingestion (Edibles): Oral consumption results in slower absorption due to gastrointestinal transit and first-pass metabolism in the liver. Peak plasma levels (<20 ng/mL) are usually reached around 120 minutes. First-pass metabolism in the liver converts THC into 11-hydroxy-THC, an active metabolite more potent than THC. It crosses the blood-brain barrier more easily and binds to CB1 receptors more efficiently (Kearn et al., 1999). Oral THC and CBD have poor bioavailability ranging from 6% to 20%.
Distribution (Lucas et al., 2018)
Cannabinoids distribute rapidly throughout the body. Due to its high lipophilicity, it crosses the blood-brain barrier and has high predilection for adipose tissue, where it can be stored for weeks in chronic users. THC and its inactive metabolite (THC-COOH) may become released from adipose tissue in response to weight loss or stress exposure (Gunasekaran et al., 2009).
THC is able to cross the placenta and is excreted in human breast milk because it is highly lipophilic.
The American Academy of Pediatrics (Ryan et al., 2018) advises against the use of THC in those who are pregnant or breastfeeding. In an analysis of two prior studies on pregnant mothers that monitored urine samples for the presence of nicotine or cannabis (Smid et al., 2022), it was found that children with intrauterine THC exposure had higher ratings on attention problem scales compared to unexposed peers, but without evidence for impairments in other cognitive domains or internalizing behaviors.
Metabolism and Elimination (Lucas et al., 2018)
THC: Metabolized predominantly in the liver by CYP2C9 and CYP3A4 enzymes into psychoactive 11-hydroxy-THC (11-OH-THC) and inactive 11-carboxy-THC (11-COOH-THC).
CBD: Metabolized mainly by CYP2C19 and CYP3A4. The pharmacologic activity of CBD metabolites are not well studied.
Smoking cannabis or tobacco induces CYP1A2, potentially influencing plasma levels of olanzapine and clozapine (see also episode 236).
Most metabolites are excreted fecally.
How Long Can THC Remain in the Body and Brain?
Plasma (Blood):
THC and its metabolites are typically detectable in plasma only several hours after a single use (Kraemer et al., 2019). However, pharmacokinetic models suggest it might persist in the plasma with as little as weekly use and perhaps longer in heavier users (Mørland & Bramness, 2020).
Urine:
The limit of quantification in a urine test for cannabis is 4 ng/mL, and the amount of time it takes until it can no longer be detected in the urine depends on the degree of consumption, as is noted in Table 1.

Note. Reprinted from “Marijuana”, by Mayo Clinic Laboratories. (n.d.). Mayo Foundation for Medical Education and Research, Table 1. Retrieved February 15, 2025, from https://news.mayocliniclabs.com/therapeutics/drug-class-testing/marijuana/
Brain and Fat Tissues:
Unlike alcohol and many other drugs that clear from the body within a few days, THC can linger for much longer—potentially weeks (Lucas et al., 2018)—due to its high lipophilicity. This means people who consistently use cannabis at least twice per week likely have some THC in their brain at all times (Mørland & Bramness, 2020). However, whether these metabolites have any functional effect remains unknown.
Chronic THC Exposure: Impact on Brain Function
PET studies of chronic, dependent cannabis users have shown lower CB1 receptor availability (by about 15-20%) throughout the brain, but this effect begins to reverse within just two days of abstinence and is normalized by four weeks (Glodosky et al., 2021; Hirvonen et al., 2011). This suggests that although THC and its metabolites may persist in the brain even after CB1 receptors normalize, their presence may not necessarily interfere with endocannabinoids or alter CB1 receptor function. This is also supported by studies of cannabis-induced cognitive impairment (deficits in attention, short term memory, verbal memory, processing speed), which improves and normalizes with increasing length of abstinence (for review, see Bourque & Potvin, 2021). However, it should be noted that the CB1 receptor is highly expressed during times of neurodevelopment, such as fetal development (Papariello et al., 2021) and again during adolescence (Meyer et al., 2018). Chronic exposure to THC during these times may downregulate these receptors and interfere with these critical periods of neurodevelopment (Lutz, 2020). One of the most contentious points in the field is whether heavy cannabis use during adolescence, or even later in life, can lead to schizophrenia by disrupting neurodevelopment during critical periods.
Cannabis, Psychosis, And Schizophrenia: A Psychiatric Risk Overview
Definition and Presentation of Cannabis Induced Psychotic Symptoms
The link between cannabis usage and psychosis is one of supreme interest to healthcare professionals and members of the public alike. When engaging in such a hotly-debated topic, it’s important to clarify the vocabulary that will be used in the discussion of said topic. Cannabis can induce psychotic symptoms, including hallucinations, paranoia, and delusions, collectively termed cannabis-associated psychotic symptoms (CAPS), as well as a more severe cannabis-induced psychotic disorder, which mimics schizophrenia with positive symptoms (e.g., hallucinations, delusions), negative symptoms (e.g., blunted affect, emotional withdrawal), and cognitive impairments like disrupted word recall (D'Souza et al., 2004; Schoeler et al., 2024). These effects, observed in controlled studies, are dose-dependent, temporary, and linked to THC administration, often resembling schizophrenia’s psychophysiologic deficits (Sherif et al., 2016). Differential diagnosis is challenging due to overlaps with primary psychotic disorders and cannabis use disorder comorbidity, with limited treatment literature and no specific guidelines; acute management involves antipsychotics, dynamic assessment, and vigilant monitoring for safety (Pauselli, 2018; Baldaçara et al., 2023).
A case report by Rossi & Beck, (2020) described a patient who presented to the emergency department with acute paranoid behavior, insomnia, and hypervigilance, which had progressively worsened over the prior month. He reported paranoid delusions involving people following him in a black truck, and had a long history of cannabis use starting at age 13 to manage self-reported anxiety. Notably, his symptoms escalated after initiating “dabbing,” a method of consuming highly concentrated cannabis with THC levels up to 80%. The onset of psychotic symptoms coincided with this change in use, leading to a diagnosis of cannabis-induced psychosis and severe cannabis use disorder. He voluntarily admitted himself for inpatient psychiatric care, was treated with risperidone, and experienced a gradual resolution of symptoms. With continued outpatient care, he tapered off medication, returned to work and college, and remained relapse-free for over a year before discontinuing psychiatric treatment.
Risk Factors For Cannabis Induced Psychotic Symptoms
It’s important to characterize what puts people at risk for experiencing psychosis in connection to cannabis usage. To this end, a large international study analyzing data from 233,475 people who use cannabis (PWUC) examined the prevalence, risk factors, and treatment circumstances surrounding cannabis-associated psychotic symptoms (CAPS) requiring emergency medical attention (Schoeler et al., 2022).
The study found that 0.47% of PWUC reported experiencing CAPS in their lifetime,
and 0.19% had experienced CAPS in the past year requiring emergency treatment.
Paranoia was the most common symptom, typically subsiding as the drug wore off.
Risk factors for CAPS included being under 21 years old (RR = 2.66), living in Denmark—possibly due to the prevalence of high-potency resin (RR = 3.01), mixing cannabis with tobacco (RR = 2.15), and using high-potency resin compared to herbal cannabis (RR = 2.11).
Individuals with existing psychiatric diagnoses, particularly psychotic disorders (RR = 14.01), bipolar disorder (RR = 4.30), anxiety (RR = 2.92), or depression (RR = 2.68), were significantly more likely to experience CAPS.
CAPS events most commonly occurred after the use of high-potency cannabis (44%) or resin (24%), even when consumed in small quantities (≤1 g in 84% of cases).
While most individuals recovered within a day, 21% reported symptoms lasting longer than four weeks.
Of those seeking emergency care, 36% were hospitalized, with admission rates highest among individuals with a history of psychosis (76%) or prolonged CAPS (54%).
CAPS in the study are comparable to rates of psychosis induced by other drugs such as alcohol-associated psychosis (around 0.4–0.7%).
Interestingly, frequency of cannabis use did not correlate with CAPS risk, possibly due to the development of tolerance. However, the study's reliance on self-reported, retrospective data and the influence of country-specific differences in cannabis use and treatment-seeking behavior limit the generalizability of its findings.
The 2023 meta-analysis by Robinson et al. addresses a major gap in the literature by quantifying psychosis risk across five levels of cannabis use frequency. Unlike previous studies that used broad categories, this analysis revealed a nuanced dose-response relationship that was most robust in a flexible non-linear model. It found no significant risk increase with yearly or monthly use, but a 35% increased risk with weekly use (RR = 1.35) and a 76% increase with daily or near-daily use (RR = 1.76), compared to non-users. The study highlights weekly use as a critical threshold for elevated psychosis risk, offering actionable insights for public health messaging to target heavy users. While the study did not assess cannabis potency or age of onset, the authors acknowledge these as important interacting risk factors.
Presentations of Other Forms of Substance-Induced Psychosis
Cannabis-induced psychosis differs in symptom presentation and severity from psychosis induced by substances like cathinone derivatives, cocaine, methamphetamine, MDMA, PCP, and ketamine.
Cathinone and its derivatives can cause psychomotor agitation, paranoia, hallucinations, and, in rare cases, excited delirium, similar to cocaine and amphetamines.
Cocaine-induced psychosis often involves paranoid delusions and auditory hallucinations.
Methamphetamine psychosis includes persecutory delusions, auditory and visual hallucinations, hostility, and disorganized thinking, but lacks negative symptoms.
MDMA psychosis features positive symptoms like delusions and hallucinations, alongside depressed mood and blunted affect.
PCP and ketamine induce psychosis with positive symptoms (hallucinations, delusions, illogical thinking) and negative symptoms (apathy, reduced speech, catatonic posturing), with PCP eliciting a stronger response (Fiorentini et al., 2021).
In contrast, cannabis-induced psychosis is characterized by heightened paranoia but less agitation and no visual hallucinations, distinguishing it from the more intense agitation and broader hallucinatory profiles of other substances.
Understanding the Limits of Current Cannabis and Psychosis Research
Challenges and Tools for Assessing Causality in Cannabis Research
Much of the research on cannabis and mental health in humans are epidemiological studies. Although epidemiological studies can provide strong evidence for associations, they are not able to fully, or often sufficiently, account for the effects of confounding variables. The most famous study that demonstrates this (discussed in episode 64) is by Di Forti and colleagues (2019), which claimed up to 12-50% of first-episode psychosis could be attributed to high potency cannabis. It was a multicenter case-control study across ten European and one Brazilian site that found an increased association between odds of first-episode psychosis and daily use of high-potency cannabis. Major limitations with regards to investigating causality included the fact that data on cannabis usages was self-reported and could not be validated using biological measures, questions pertaining to cannabis usage were unable to assess potency, and recruitment of controls and patients were not random, as well as other factors. The population attributable fractions were calculated assuming causality, which has not been established in the study, much less the overall body of literature. Gillespie and colleagues (2019) argued in response to Di Forti et al. that their analysis did not adequately account for the genetic correlation between schizophrenia and cannabis use (previously identified at r = 0.25), nor sufficiently address the alternative hypothesis supported by their bidirectional Mendelian randomization study, which indicated that causality might predominantly flow from schizophrenia to cannabis use, rather than vice versa.
To help assess if a relationship in epidemiology is causal or not, the Bradford Hill Criteria can be of much use. They are a series of nine points that are commonly utilized to assess causality within epidemiology (Shimonovich et al., 2021). They are qualities intended to be kept in mind when assessing if a connection is due to something besides causality, as opposed to definitive rules that must all be checked off before a connection is deemed to be causal in nature. They can be quite helpful when evaluating the strength of studies as well as their claims of causal connections. These criteria are listed below, with commentary about their modern importance:
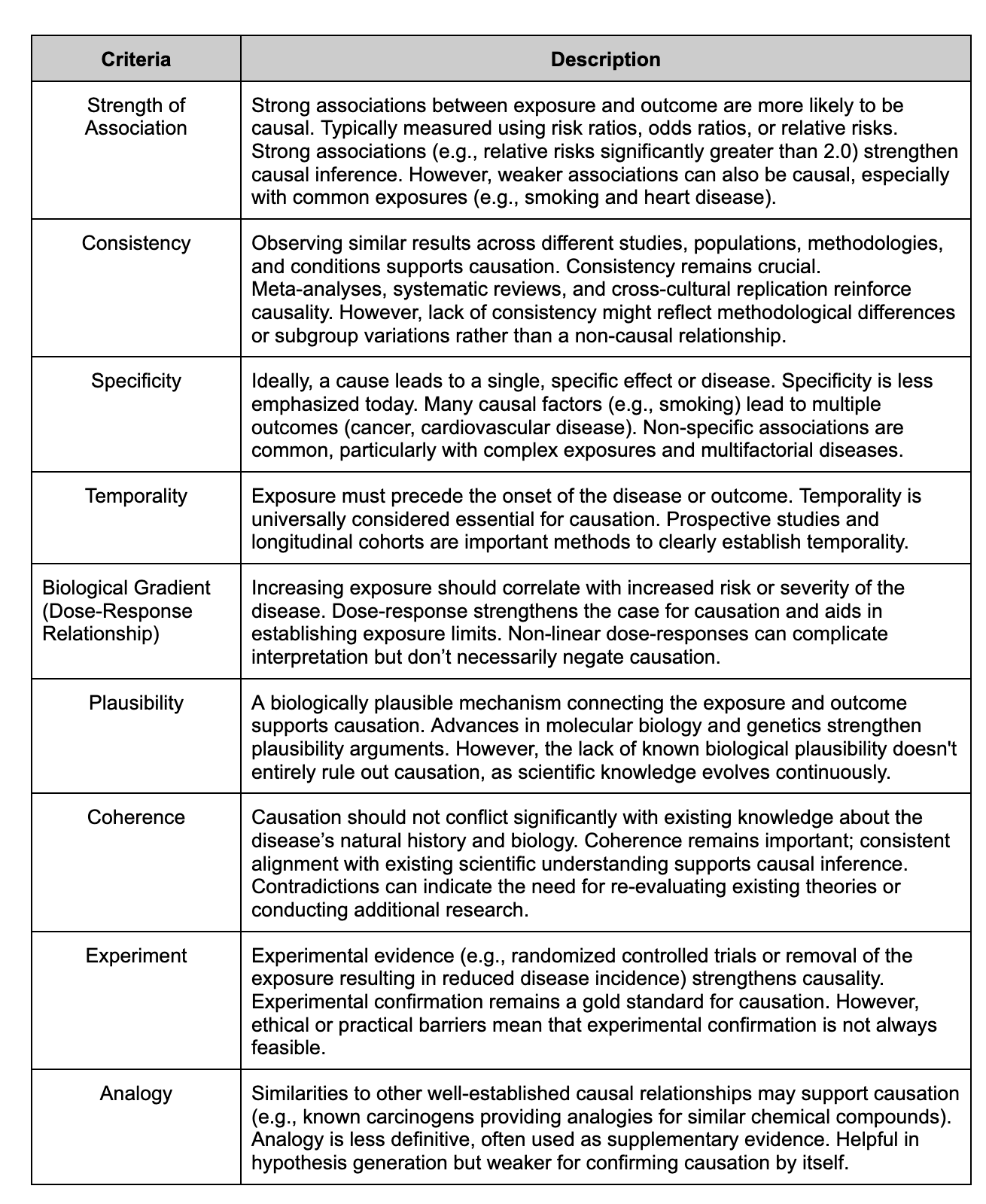
The nine criteria that constitute the Bradford Hill Criteria.
Examples of Prospective Studies Investigating Cannabis Use and Psychosis
To adequately address whether the effects of cannabis use in adolescence is causally related to schizophrenia, more prospective studies are needed. Studies, like the prospective historical cohort study by Zammit et al. (2002), which investigated the causal link between adolescent cannabis use and schizophrenia, utilizing data from a 1969-70 survey of 50,087 Swedish male conscripts (aged 18-20), representing over 97% of the country’s male population in that age group. The study employed a prospective longitudinal design, assessing cannabis use through structured interviews with psychologists and psychiatrists, diagnosing psychiatric conditions per ICD-8 criteria, and following subjects from 1970 to 1996.
Potential confounders adjusted for included:
psychiatric diagnosis at conscription
IQ
personality traits
upbringing
paternal age
cigarette smoking
childhood behavior
alcohol misuse
family psychiatric history
financial situation
father’s occupation
The study found a dose-dependent association between cannabis use frequency and schizophrenia risk, with an adjusted odds ratio (OR) of 1.5 (95% CI 1.1-2.0) for lifetime use and 3.1 (1.7-5.5) for heaviest use (>50 occasions).
Among 1648 subjects using only cannabis, 1.1% developed schizophrenia, with a higher risk (adjusted OR 1.9, 1.1-3.1) compared to non-users.
5.7% of those cannabis users who developed schizophrenia (4/70) used >50 times.
No association was found with other psychotic disorders, suggesting specificity to schizophrenia.
Although the study supports a possible causal connection due to its dose-dependent findings and rigorous adjustments, a key limitation is the low base rate of schizophrenia in the sample (0.71%), which may reflect the exclusion of individuals with psychiatric disorders at baseline.
A prospective population-based study by van Os et al. (2002) followed over 4,000 adults (ages 18–64) in the Netherlands who were free of psychosis at baseline and found that baseline cannabis use predicted later development of psychotic symptoms, including symptoms severe enough to require mental health care.
The odds of developing pathology-level psychosis were over 24 times higher (OR = 24.17) in those who had used cannabis at baseline, compared to non-users even after controlling for age, sex, education, ethnicity, urbanicity, and discrimination.
However, the OR of 24 here is also based on a sensitivity analysis, where those cases of psychosis at follow up are imputed because they lost so many people to follow up.
In the other sensitivity analyses when they imputed missing participant cases differently, the authors only found an OR of 3.
Also, while they controlled for baseline psychotic symptoms and age, it's likely that the people who were experiencing psychotic symptoms at the follow up clinical interview had a psychotic disorder at baseline.
Importantly, the study claimed that there was a dose-response effect, in that greater cumulative use was associated with progressively higher risk. However, it is difficult to accurately assess dose response with only 10 cases and 4 categories of use severity.
The authors also showed that cannabis use predicted psychosis independently of other substances like stimulants and psychedelics, and that cannabis use at baseline was a stronger predictor than more recent use, suggesting a temporal relationship.
Furthermore, for those with an existing vulnerability to psychosis at baseline, cannabis use led to dramatically higher rates of poor outcomes, with 80% of psychosis cases in this group attributable to the synergistic effect of cannabis and baseline vulnerability.
These findings address some of the Bradford Hill criteria, including specificity, and biological gradient (dose-response) —and adds to the supporting evidence that cannabis may play a causal role in the development or exacerbation of psychosis.
Can Cannabis-Induced Psychosis Lead To Schizophrenia? What The Research Says
The question of whether or not cannabis usage leads to long term psychosis or schizophrenia has been the subject of debate and research for decades. There have been recent studies looking at modern trends relating to cannabis usage potentially transitioning to long-term schizophrenia. A recent population-based cohort study from Ontario, Canada (Myran et al., 2025a) reported a significant increase in the population-attributable fraction (PARF) of schizophrenia linked to cannabis use disorder (CUD) following cannabis legalization. However, the study’s methodology defined CUD solely by emergency department visits or inpatient psychiatric admissions related to cannabis use, excluding outpatient cases. This flawed definition likely biased the results by capturing a subset of individuals already at higher risk for schizophrenia due to genetic or psychological predispositions. Furthermore, while cannabis use increased post-legalization, the incidence of schizophrenia actually declined by 27.2% between 2006 and 2022, contradicting the study’s projections. A related study using the same cohort (Myran et al., 2025b) found CUD associated with higher all-cause mortality (HR 2.79), but it relied on the same narrow and problematic definition of CUD. The subgroup defined as having CUD was more likely to be socioeconomically disadvantaged, have co-occurring mental health disorders, and use other substances, introducing substantial confounding variables. As a result, both studies’ conclusions are undermined by methodological limitations and confounding factors, making it difficult to isolate cannabis use as the primary driver of schizophrenia risk or increased mortality.
A 2023 retrospective cohort study of electronic medical records from the same cohort of nearly 10 million Ontario residents aged 14–65, excluding those with prior psychotic diagnoses, investigated the 3-year risk of transitioning to psychosis following emergency department (ED) visits for substance use or substance-induced psychosis, compared to the general population, while controlling for confounders like age, sex, neighborhood income, rurality, and prior mental health care (Myran et al., 2023).
Of the 9,844,497 individuals, 407,737 (4.1%) had ED visits for substance use
13,784 (0.1% of the total population) presented with substance-induced psychosis
Of whom 18.5% developed a chronic psychotic disorder within 3 years.
The adjusted hazard ratio (aHR) for transitioning to schizophrenia spectrum disorder was significantly elevated for substance-induced psychosis (aHR 62.0; 95% CI, 58.8–65.4) and substance use without psychosis (aHR 4.8; 95% CI, 4.6–5.0), with cannabis-induced psychosis showing the highest risk (aHR 84.9; 95% CI, 78.7–91.6) when compared to other substances such as:
amphetamines (22.3)
cocaine (16.6)
alcohol (16.3)
or polysubstance use (48.8)
Younger age and male sex further increased risk.
Despite adjustments, residual confounding likely persisted due to baseline differences, such as higher prior acute care for substance use among those with substance-induced psychosis (37% vs. 8.5% for non-psychosis substance use and 1.2% for the general population), and the occasional binary treatment of mental health care variables oversimplified complex histories.
This small subset (0.1% of the population) with substance-induced psychosis had more comorbidities, limiting generalizability to typical cannabis users, and the retrospective design could not address reverse causality or many other Bradford-Hill criteria, though it highlighted cannabis-induced psychosis as a stronger risk factor for psychotic disorders than psychosis induced by other substances.

Table 3. Risk of Transition to Schizophrenia Spectrum Disorder Within 3 Years Based on Age, Sex, and Substance Use.
Note. Reprinted from “Transition to schizophrenia spectrum disorder following emergency department visits due to substance use with and without psychosis”, by Myran et al., 2023, JAMA Psychiatry, 80(11), Table 3.
Explaining the Cannabis-Schizophrenia Connection: Three Leading Hypotheses
There are three main lines of thinking in the literature to explain the association between cannabis and schizophrenia (Hamilton & Monaghan, 2019).
The first hypothesis is that cannabis is causally associated with schizophrenia; this is based on multiple studies supporting the claim that frequent, high-dose cannabis use is associated with the development of psychosis, and the fact that cannabis can induce psychotic symptoms in those without a history of psychosis.
The second hypothesis is that people with schizophrenia use cannabis at a higher rate to self-medicate negative symptoms.
The last is that cannabis increases risk for psychosis in people who are already at risk due to genetic and environmental factors.
Hypothesis #1: Cannabis is Causally Associated with Schizophrenia
The Impact of Cannabis on the Developing Adolescent Brain
The endocannabinoid system plays a significant role in neurodevelopment by modulating synaptic strength and plasticity. Notably, CB1 receptor expression is highest during fetal and adolescent neurodevelopment. Heavy cannabis use during adolescence may downregulate these receptors during critical periods of synaptic pruning, potentially leading to lasting neurodevelopmental changes that increase susceptibility to psychosis. In rodent models, chronic THC exposure during adolescence has been shown to disrupt synaptic pruning, leading to premature dendritic atrophy or functional alterations in cortical glutamatergic pyramidal neurons—morphological changes that resemble those seen in schizophrenia and induced by chronic stress (Miller et al., 2019). This may stem from THC-induced impairments in specific subpopulations of GABAergic interneurons, particularly those containing parvalbumin and CCK (Renard et al., 2017). Schizophrenia is also associated with dysregulation of parvalbumin and somatostatin interneurons (Vid Prkačin et al., 2023).
How Cannabis Use During Adolescence Affects Brain Structure
Structural MRI studies also tend to show some commonalities between chronic cannabis use and schizophrenia, mainly reduced right hippocampal volume. However, early studies typically do not control for the effects of early life adversity (Battistella et al., 2014), an independent factor affecting hippocampal volume, and the observed effects often disappear when controlling for alcohol use (Matochik et al., 2005; Weiland et al., 2015). However, in a study by Chye et al. (2019), people with cannabis use disorder exhibited reduced hippocampal volume even after adjusting for alcohol use. Further, a large-scale study of over 1000 participants (Owens et al., 2021) showed that people with recent cannabis use, as measured by positive THC urine tests, had bilateral reductions in hippocampal volume, whereas “effects may dissipate following prolonged abstinence” (Owens et al., 2021, Abstract ). A meta-analysis of 16 studies found no evidence that heavy cannabis use during adolescence or young adulthood leads to structural changes in cortical or subcortical gray matter or white matter integrity (Lorenzetti et al., 2023), but there was a trend for decreased PFC volume or thickness that warrant larger studies.

Note. Reprinted from “Brain Anatomical Alterations in Young Cannabis Users: Is it All Hype? A Meta-Analysis of Structural Neuroimaging Studies”, by Lorenzetti et al., 2023, Cannabis and cannabinoid research, 8(1), Figure 4, p. 191.
The authors concluded that “while prolonged and long-term exposure to heavy cannabis use may be required to detect gross volume alterations, more studies in young cannabis users are needed to map in detail cannabis-related neuroanatomical changes.” A separate review by Levine and colleagues (2017) noted that some studies did not assess brain changes over time, simply observing the brains of adolescents who used cannabis vs. those who did not. This led the authors to conclude, “It remains unclear whether the neuroanatomical and functional abnormalities are caused by, or exist prior to, the onset of cannabis exposure.”
However, the largest longitudinal study of adolescents to date, conducted by Albaugh and colleagues (2021) using the IMAGEN cohort, provides a more nuanced picture:
800 European participants received fMRI scans at ages 14 (prior to any substantial cannabis use) and 19 (after possible initiation).
There was a dose-dependent association between cannabis consumption and accelerated cortical thinning by age 19—most pronounced in prefrontal regions densely populated with CB1 receptors.
Importantly, no baseline differences in cortical thickness predicted future cannabis use, suggesting these neuroanatomical changes were likely driven by exposure rather than pre-existing traits.
Further analysis from the same cohort at age ~23–24 showed that initiating cannabis use during adolescence produced distinctly greater changes in frontal cortical development compared to onset in the twenties (Albaugh et al., 2023).
Cannabis Use in Adolescence and its Influences on Brain Activity
fMRI studies examining resting-state activity and cognitive task performance have linked heavy cannabis use to altered activity and connectivity in brain regions involved in cognitive control and executive functioning (e.g., dlPFC, anterior cingulate, OFC). However, findings regarding the directionality of these changes (increased vs. decreased activity) remain inconsistent (Hammond et al., 2022; Harding et al., 2012). It is also unclear whether these alterations persist after abstinence or if they predate cannabis use, in which case they might serve as markers of vulnerability to both cannabis use and schizophrenia.
Additionally, while cannabis is often associated with dopamine dysregulation, a systematic review of nine fMRI studies using the monetary incentive delay task found no significant differences in reward-related brain responses among daily cannabis users. But this narrowly focused summary fails to acknowledge broader evidence from other paradigms and modalities like PET studies and neuromelanin-sensitive MRI (Beyer et al., 2024). However, people with cannabis use disorder (CUD) exhibit increased neuromelanin levels, as evidenced by elevated neuromelanin-sensitive MRI signals, particularly within specific ventral substantia nigra/ventral tegmental area (SN/VTA) voxels previously associated with heightened psychosis severity, suggesting elevated dopamine function related to cannabis use (Ahrens et al., 2025). Furthermore, some studies do suggest cannabis use in adolescence changes reward responsivity, increasing risk for anhedonia; however, other studies using different methodologies don’t support this finding.
Hypothesis #2: People With Schizophrenia Use Cannabis at a Higher Rate to Self-Medicate Negative Symptoms
Nearly half of people with schizophrenia develop a CUD in their lifetime (Ahmed et al., 2021). Some patients report that it helps with negative symptoms related to volition, affect, and poverty of thought. However, a systematic review and meta-analysis found no difference in negative symptoms between schizophrenic patients who used cannabis and those who did not (Sabe et al., 2020).
Hypothesis #3: Cannabis Increases Risk for Psychosis in People Who Are Already At Risk Due To Genetic and Environmental Factors
Overlapping Genetics Between Cannabis Use Disorder and Schizophrenia: What We Know
Heritability estimates for cannabis use disorder and schizophrenia are about 50% and 80% respectively (Chenoweth, 2024), suggesting both disorders are highly heritable. Considering the higher comorbidity between the two disorders, many have argued there is a genetic overlap. Some studies do suggest that people with schizophrenia and their healthy relatives experience greater rewarding effects or sensitivity to cannabis (Kuepper et al., 2013), which may suggest cannabis is more likely to be the drug of choice in people with schizophrenia (similar to nicotine). What’s unclear, however, is whether this effect is specific to cannabis, as people with schizophrenia are also more likely to use other illicit drugs.
Early research into the relationship between cannabis use disorder and schizophrenia often focused on candidate genes—specific genetic variants believed to interact with environmental factors (like adolescent cannabis use) to increase the risk of psychosis. Among these genes were COMT, which influences dopamine regulation (Caspi et al., 2005), AKT1, involved in glucose metabolism (Di Forti et al., 2012), and CNR1 (cannabinoid receptor gene, Benyamina et al., 2011). Some small-sample studies reported that adolescents carrying certain polymorphisms of these genes are at higher risk of developing schizophrenia if they begin using cannabis at a young age (Caspi et al., 2005; Di Forti et al., 2012). However, because candidate gene studies often use limited samples (thus limiting their power) and are prone to publication bias, replication has been inconsistent (Verweij et al., 2022). Therefore, the true effect size of any single gene in moderating the risk of developing schizophrenia due to cannabis use is minimal and the relationship between cannabis use and schizophrenia is influenced by multiple genes.
Because of this, Genome-Wide Association Studies (GWAS) are more commonly used now, as they screen the entire genome for common variants associated with schizophrenia or cannabis use in large samples (Verweij et al., 2017). These genes that are consistently associated with increased risk can be compiled to give polygenic risk scores for each of these outcomes. The polygenic risk scores that predict cannabis use can then be used to test whether they confer greater risk of schizophrenia. This type of study is called Mendelian randomization and allows for researchers to assess whether samples with high genetic risk for cannabis use are more likely to develop schizophrenia, even in the absence of actual cannabis use. One Mendelian randomization analysis found a causal effect of cannabis use on schizophrenia (Vaucher et al., 2018), while three others suggest reverse causation, in which genetic liability for schizophrenia predicts greater cannabis use or cannabis use disorder (Gage et al., 2017; Johnson et al., 2021; Pasman et al., 2018) and another study detected no clear evidence of a causal link between cannabis use and schizophrenia (Jang et al., 2022).
However, these studies require more robust and diverse sampling methods, a consistent and dose-related measurement of cannabis use, and clearer strategies to address the potential violations of Mendelian randomization assumptions—particularly pleiotropy (where one set of genetic variants can influence multiple traits associated with both schizophrenia and cannabis use). Because schizophrenia and CUD share overlapping genetic architectures, it is difficult to confirm whether specific variants are truly exerting causal effects or are influencing traits common to both disorders (i.e., horizontal pleiotropy), such as impulsivity, neuroticism (see also Episode 92), executive function, neurodevelopment, etc. (Johnson et al., 2024; Richter et al., 2019). Variants in genes related to the endocannabinoid system, glutamate signaling, dopamine, or stress sensitivity may act across these domains, complicating any causal inferences drawn from Mendelian randomization studies (Johnson et al., 2024; Richter et al., 2019 for specific genes discussed in the podcast).
Adverse Childhood Experiences (ACEs) Increase Risk for Both Cannabis Use Disorder and Schizophrenia
Adverse Childhood Experiences (ACEs) are significant early-life stressors, including abuse, neglect, and household dysfunction, that increase the risk of both cannabis use and schizophrenia (see also episodes 203, 204, 217). Individuals with four or more ACEs face a substantially heightened risk for both substance use disorders–including CUD–in adolescence and later in life, and psychotic disorders.
ACEs are associated with lasting neurobiological changes, such as dysregulation of the HPA axis, increased systemic inflammation, reduced hippocampal volume, anhedonia, and increased amygdala reactivity to negative emotions. These alterations, combined with cannabis use—especially during critical developmental periods—may amplify the risk of psychosis.
It is important to recognize that most people who began using cannabis at an early age are more likely to have lived in unstable home environments with greater substance use and less parental oversight, which needs to be taken into account when interpreting studies of people who began using cannabis at a young age.
Cannabis Use and Risk of Psychotic Relapse in Schizophrenia
Regardless of whether or not cannabis causes schizophrenia, it is evident from clinical experience and the literature that cannabis use can be incredibly destabilizing for patients who have a psychotic disorder. In the review of human laboratory studies mentioned earlier (Sherif et al., 2016), as well as a double-blind RCT (D'Souza et al., 2005) that compared the effects of intravenous THC vs. a placebo treatment in patients with schizophrenia spectrum disorder, it was shown that THC worsens symptoms of psychosis in a manner that is transient and dependent on the dosage.
However, the data on whether or not cannabis causes schizophrenia is mixed. A large 2023 individual participant data meta-analysis by Argote et al., using PANSS scores from over 3,000 individuals with schizophrenia spectrum disorders, offered more nuanced insight into how cannabis use affects symptom profiles. After adjusting for key confounders (e.g., age, sex, illness duration, substance use), cannabis users exhibited significantly higher severity of positive symptoms (adjusted mean difference [aMD] = 0.38) and greater excitement symptoms (aMD = 0.16), but lower severity of negative symptoms (aMD = -0.50) compared to non-users. No association was found with disorganization or depressive symptoms. These results support the clinical observation that cannabis can exacerbate paranoid ideation and hyperactivation, while simultaneously appearing to attenuate negative symptoms like avolition or affective flattening. However, the authors caution that these findings do not imply causality and may reflect a self-selection effect, where individuals with fewer negative symptoms are more likely to use substances. Nevertheless, this study strengthens prior findings that continued cannabis use worsens positive symptom trajectories, and highlights the importance of differentiating symptom clusters when assessing cannabis impact. In a different meta-analysis that aimed to determine the impact of cannabis use on the efficacy of antipsychotic dosage, the evolution of symptoms, therapeutic resistance, and the risk of relapse in patients with schizophrenia who are taking medication (Rault et al., 2022), cannabis use was not shown to be associated with poorer symptoms evolution but was shown to be associated with higher relapse rates.
This ties into one of the more important points with regards to cannabis use in patients with schizophrenia. Over the long term, symptoms may or may not be worse, but cannabis use will lead to more relapses, which is a serious problem given the nature of a relapse into psychosis. Possible explanations for this include the fact that patients who continue using cannabis and have more relapses might have worse schizophrenia symptoms at baseline, are more likely to be noncompliant on medications, or are experiencing more life stress. These possibilities were addressed by a prospective, longitudinal study by Scheffler et al. (2021) followed 98 patients with first-episode schizophrenia spectrum disorders over 24 months while on long-acting injectable antipsychotics, allowing for reliable assessment of medication compliance. Participants were divided into cannabis users (n=45) and non-users (n=53) and relapse was defined by specific increases in PANSS scores or CGI worsening. While both groups showed similar baseline psychotic symptoms (F=0.448, p=0.7), cannabis users exhibited poorer social and occupational functioning initially (p=0.008). Importantly, cannabis users experienced significantly more relapses (22.2% vs. 7.5%, p=0.039), despite similar rates of remission (76% for cannabis users vs. 83% for non-users). Furthermore, frequency of cannabis use, verified by urine toxicology, predicted relapse (ß=0.47, p=0.03). Despite similar symptom remission rates over time, the study suggests a dose-dependent relationship between cannabis use and relapse risk, potentially due to cannabis lowering the threshold for psychotic episodes or interacting with antipsychotic metabolism through the CYP450 system (Smith & Gruber, 2023). However, a literature review by Rault and colleagues (2022) found no evidence that cannabis use necessitates higher antipsychotic doses, suggesting it may not increase antipsychotic resistance. Notably, the Scheffler study effectively controlled for key confounds—baseline symptom severity and medication noncompliance—strengthening its conclusion that ongoing cannabis use elevates relapse risk independently of these factors.
Conclusion Regarding Cannabis And Psychosis
We’re living in an unprecedented era of cannabis use in North America. With legalization sweeping across most U.S. states—and only four now maintaining full prohibition—cannabis has become widely accessible, increasingly potent, and culturally normalized. Today’s products are far from the cannabis of the past: THC concentrations now regularly exceed 17–28%, with some concentrates reaching above 90% (Backman, 2023). Alongside this rise in potency is a shift in perception. Dispensaries promote cannabis as a natural remedy for anxiety, insomnia, and depression. Among young adults, cannabis is increasingly seen as a healthy alternative to alcohol—and for the first time in U.S. history, the number of daily cannabis users (17.7 million) has surpassed daily alcohol users (14.7 million) (Caulkins, 2024).
But those of us in clinical practice are seeing a different side of the story. Many of us have cared for patients experiencing cannabis-induced psychosis: young people arriving in the emergency department with paranoia, hallucinations, and delusions after consuming high-potency THC products. Others with schizophrenia relapse after prolonged stability—often following renewed cannabis use. These cases are becoming increasingly common, reinforcing what many psychiatrists now believe: cannabis is one of several environmental risk factors that can unmask or exacerbate psychotic disorders.
Frustratingly, the pace of research has failed to match the public’s growing use. Regulatory barriers restrict access to the very products people are using, while ethical limitations hinder the ability to conduct randomized controlled trials. As a result, most available data come from observational studies—which, while valuable, often struggle to account for confounding variables such as genetic risk, Adverse Childhood Experiences (ACEs), co-occurring substance use, and social adversity.
In this episode, we critically examined the existing literature through the lens of the Bradford Hill criteria. While numerous epidemiological studies demonstrate a consistent association between cannabis use and psychosis—with cannabis being associated with the highest risk of transition from substance-induced psychosis to schizophrenia compared to other substances—causality still remains difficult to “prove”. For example, a Swedish cohort of over 50,000 conscripts found that those who had used cannabis more than 50 times had more than triple the odds of later developing schizophrenia (Zammit et al., 2002), but even this rigorous design cannot fully isolate cannabis from other risk factors. However, regardless of whether cannabis is causally associated with the development of psychosis, it may still act as a catalyst for psychosis and other mental health problems in individuals with genetic or environmental vulnerabilities.
As the normalization of cannabis use accelerates and research struggles to keep pace, we find ourselves at a critical juncture. We as mental health professionals must remain informed and engaged to connect with our patients and the public. It is our responsibility to serve as trusted resources of critical discussion in an era where cannabis is marketed as a cure-all, often without regard for psychiatric risk. We must also advocate for more rigorous, unbiased research to ensure that public education and drug policy is grounded in science—not sentiment—and that we help shape the cultural narrative around cannabis in the critical years ahead.
We hope this episode has equipped you for future discussions about cannabis with patients, families, and colleagues and that you tune in for the next part of the series, where we will discuss cannabis and depression, anxiety, PTSD, cognition, and more.
References:
Ahmed, S., Roth, R. M., Stanciu, C. N., & Brunette, M. F. (2021). The impact of THC and CBD in schizophrenia: A systematic review. Frontiers in Psychiatry, 12, 694394. https://doi.org/10.3389/fpsyt.2021.694394
Ahrens, J., Ford, S. D., Schaefer, B., Reese, D., Khan, A. R., Tibbo, P., Rabin, R., Cassidy, C. M., & Palaniyappan, L. (2025). Convergence of cannabis and psychosis on the dopamine system. JAMA Psychiatry. Advance online publication. https://doi.org/10.1001/jamapsychiatry.2025.0432
Albaugh, M. D., Ottino-Gonzalez, J., Sidwell, A., Lepage, C., Juliano, A., Owens, M. M., Chaarani, B., Spechler, P., Fontaine, N., Rioux, P., Lewis, L., Jeon, S., Evans, A., D’Souza, D., Radhakrishnan, R., Banaschewski, T., Bokde, A. L. W., Quinlan, E. B., Conrod, P., ... Garavan, H. (2021). Association of cannabis use during adolescence with neurodevelopment. JAMA Psychiatry. Advance online publication. https://doi.org/10.1001/jamapsychiatry.2021.1258
Albaugh, M. D., Owens, M. M., Juliano, A., Ottino-Gonzalez, J., Cupertino, R., Cao, Z., Mackey, S., Lepage, C., Rioux, P., Evans, A., Banaschewski, T., Bokde, A. L. W., Conrod, P., Desrivières, S., Flor, H., Grigis, A., Gowland, P., Heinz, A., Ittermann, B., … IMAGEN Consortium. (2023). Differential associations of adolescent versus young adult cannabis initiation with longitudinal brain change and behavior. Molecular Psychiatry, 28(11), 5173–5182. https://doi.org/10.1038/s41380-023-02148-2
Argote, M., Sescousse, G., Brunelin, J., Baudin, G., Schaub, M. P., Rabin, R., Schnell, T., Ringen, P. A., Andreassen, O. A., Addington, J. M., Brambilla, P., Delvecchio, G., Bechdolf, A., Wobrock, T., Schneider-Axmann, T., Herzig, D. A., Mohr, C., Vila-Badia, R., Usall, J., … Rolland, B. (2023). Association between cannabis use and symptom dimensions in schizophrenia spectrum disorders: An individual participant data meta-analysis on 3053 individuals. eClinicalMedicine, 64, 102199. https://doi.org/10.1016/j.eclinm.2023.102199
Arkell, T. R., Kevin, R. C., Vinckenbosch, F., Lintzeris, N., Theunissen, E., Ramaekers, J. G., & McGregor, I. S. (2022). Sex differences in acute cannabis effects revisited: Results from two randomized, controlled trials. Addiction biology, 27(2), e13125. https://doi.org/10.1111/adb.13125
Backman, I. (2023, August 30). Not your grandmother’s marijuana: Rising THC concentrations in cannabis can pose devastating health risks. Yale School of Medicine. https://medicine.yale.edu/news-article/not-your-grandmothers-marijuana-rising-thc-concentrations-in-cannabis-can-pose-devastating-health-risks/
Baldaçara, L., Ramos, A., & Castaldelli-Maia, J. M. (2023). Managing drug-induced psychosis. International Review of Psychiatry, 35(5–6), 496–502. https://doi.org/10.1080/09540261.2023.2261544
Bassir Nia, A., Bender, R., & Harpaz-Rotem, I. (2019). Endocannabinoid system alterations in posttraumatic stress disorder: A review of developmental and accumulative effects of trauma. Chronic Stress, 3, 1–10. https://doi.org/10.1177/2470547019864096
Battistella, G., Fornari, E., Annoni, J. M., Chtioui, H., Dao, K., Fabritius, M., Favrat, B., Mall, J. F., Maeder, P., & Giroud, C. (2014). Long-term effects of cannabis on brain structure. Neuropsychopharmacology : official publication of the American College of Neuropsychopharmacology, 39(9), 2041–2048. https://doi.org/10.1038/npp.2014.67
Benyamina, A., Kebir, O., Blecha, L., Reynaud, M., & Krebs, M.-O. (2011). CNR1 gene polymorphisms in addictive disorders: A systematic review and a meta-analysis. Addiction Biology, 16(1), 1–6. https://doi.org/10.1111/j.1369-1600.2009.00198.x
Beyer, E., Poudel, G., Antonopoulos, S., Thomson, H., & Lorenzetti, V. (2024). Brain reward function in people who use cannabis: A systematic review. Frontiers in Behavioral Neuroscience, 17, 1323609. https://doi.org/10.3389/fnbeh.2023.1323609
Bourque, J., & Potvin, S. (2021). Cannabis and cognitive functioning: From acute to residual effects, from randomized controlled trials to prospective designs. Frontiers in Psychiatry, 12, 596601. https://doi.org/10.3389/fpsyt.2021.596601
Caspi, A., Moffitt, T. E., Cannon, M., McClay, J., Murray, R., Harrington, H., Taylor, A., Arseneault, L., Williams, B., Braithwaite, A., Poulton, R., & Craig, I. W. (2005). Moderation of the effect of adolescent-onset cannabis use on adult psychosis by a functional polymorphism in the catechol-O-methyltransferase gene: Longitudinal evidence of a gene × environment interaction. Biological Psychiatry, 57(10), 1117–1127. https://doi.org/10.1016/j.biopsych.2005.01.026
Caulkins, J. P. (2024). Changes in self-reported cannabis use in the United States from 1979 to 2022. Addiction, 119(9), 1648–1652. https://doi.org/10.1111/add.16519
Chenoweth, M. J. (2024). Cracking the chicken and egg problem of schizophrenia and substance use: Genetic interplay between schizophrenia, cannabis use disorder, and tobacco smoking. Neuropsychopharmacology, 49, 1653–1654. https://doi.org/10.1038/s41386-024-01898-z
Chye, Y., Lorenzetti, V., Suo, C., Batalla, A., Cousijn, J., Goudriaan, A. E., Jenkinson, M., Martin-Santos, R., Whittle, S., Yücel, M., & Solowij, N. (2019). Alteration to hippocampal volume and shape confined to cannabis dependence: A multi-site study. Addiction Biology, 24(5), 822–834. https://doi.org/10.1111/adb.12652
Cohen, Y., Kolodziej, A., & Morningstar, M. (2024). Seventeen years since rimonabant's downfall: Reassessing its suicidality risk profile. Obesity (Silver Spring), 32(7), 1235–1244. https://doi.org/10.1002/oby.24019
Di Forti, M., Iyegbe, C., Sallis, H., Kolliakou, A., Falcone, M. A., Paparelli, A., Sirianni, M., La Cascia, C., Stilo, S. A., Marques, T. R., Handley, R., Mondelli, V., Dazzan, P., Pariante, C., David, A. S., Morgan, C., Powell, J., & Murray, R. M. (2012). Confirmation that the AKT1 (rs2494732) genotype influences the risk of psychosis in cannabis users. Biological Psychiatry, 72(10), 811–816. https://doi.org/10.1016/j.biopsych.2012.06.020
Di Forti, M., Quattrone, D., Freeman, T. P., Tripoli, G., Gayer-Anderson, C., Quigley, H., Rodriguez, V., Jongsma, H. E., Ferraro, L., La Cascia, C., La Barbera, D., Tarricone, I., Berardi, D., Szöke, A., Arango, C., Tortelli, A., Velthorst, E., Bernardo, M., Marta Del-Ben, C., ... Murray, R. M. (2019). The contribution of cannabis use to variation in the incidence of psychotic disorder across Europe (EU-GEI): A multicentre case-control study. The Lancet Psychiatry, 6(5), 427–436. https://doi.org/10.1016/S2215-0366(19)30048-3
DISA Global Solutions. (2025, April 28). Marijuana legality by state. https://disa.com/marijuana-legality-by-state
D'Souza, D. C., Perry, E., MacDougall, L., Ammerman, Y., Cooper, T., Wu, Y. T., Braley, G., Gueorguieva, R., & Krystal, J. H. (2004). The psychotomimetic effects of intravenous delta-9-tetrahydrocannabinol in healthy individuals: Implications for psychosis. Neuropsychopharmacology, 29(8), 1558–1572. https://doi.org/10.1038/sj.npp.1300496
D’Souza, D. C., Abi-Saab, W. M., Madonick, S., Forselius-Bielen, K., Doersch, A., Braley, G., Gueorguieva, R., Cooper, T. B., & Krystal, J. H. (2005). Delta-9-tetrahydrocannabinol effects in schizophrenia: Implications for cognition, psychosis, and addiction. Biological Psychiatry, 57(6), 594–608. https://doi.org/10.1016/j.biopsych.2004.12.006
Englund, A., Morrison, P. D., Nottage, J., Hague, D., Kane, F., Bonaccorso, S., Stone, J. M., Reichenberg, A., Brenneisen, R., Holt, D., Feilding, A., Walker, L., Murray, R. M., & Kapur, S. (2013). Cannabidiol inhibits THC-elicited paranoid symptoms and hippocampal-dependent memory impairment. Journal of psychopharmacology (Oxford, England), 27(1), 19–27. https://doi.org/10.1177/0269881112460109
Englund, A., Oliver, D., Chesney, E., Chester, L., Wilson, J., Sovi, S., De Micheli, A., Hodsoll, J., Fusar-Poli, P., Strang, J., Murray, R. M., Freeman, T. P., & McGuire, P. (2023). Does cannabidiol make cannabis safer? A randomised, double-blind, cross-over trial of cannabis with four different CBD:THC ratios. Neuropsychopharmacology, 48, 869–876. https://doi.org/10.1038/s41386-022-01478-z
Fiorentini, A., Cantù, F., Crisanti, C., Cereda, G., Oldani, L., & Brambilla, P. (2021). Substance-induced psychoses: An updated literature review. Frontiers in Psychiatry, 12, 694863. https://doi.org/10.3389/fpsyt.2021.694863
Gage, S. H., Jones, H. J., Burgess, S., Bowden, J., Davey Smith, G., Zammit, S., & Munafò, M. R. (2017). Assessing causality in associations between cannabis use and schizophrenia risk: a two-sample Mendelian randomization study. Psychological Medicine, 47(5), 971–980. doi:10.1017/S0033291716003172
Gillespie, N. A., Pasman, J. A., Treur, J. L., Derks, E. M., Verweij, K. J. H., & Vink, J. M. (2019). High-potency cannabis and incident psychosis: Correcting the causal assumption. The Lancet Psychiatry, 6(6), 464. https://doi.org/10.1016/S2215-0366(19)30174-9
Glodosky, N. C., Cuttler, C., & McLaughlin, R. J. (2021). A review of the effects of acute and chronic cannabinoid exposure on the stress response. Frontiers in neuroendocrinology, 63, 100945. https://doi.org/10.1016/j.yfrne.2021.100945
Gunasekaran, N., Long, L. E., Dawson, B. L., Hansen, G. H., Richardson, D. P., Li, K. M., Arnold, J. C., & McGregor, I. S. (2009). Reintoxication: the release of fat-stored delta(9)-tetrahydrocannabinol (THC) into blood is enhanced by food deprivation or ACTH exposure. British journal of pharmacology, 158(5), 1330–1337. https://doi.org/10.1111/j.1476-5381.2009.00399.x
Hamilton, I., & Monaghan, M. (2019). Cannabis and psychosis: Are we any closer to understanding the relationship? Current Psychiatry Reports, 21(48). https://doi.org/10.1007/s11920-019-1044-x
Hammond, C. J., Allick, A., Park, G., Rizwan, B., Kim, K., Lebo, R., Nanavati, J., Parvaz, M. A., & Ivanov, I. (2022). A Meta-Analysis of fMRI Studies of Youth Cannabis Use: Alterations in Executive Control, Social Cognition/Emotion Processing, and Reward Processing in Cannabis Using Youth. Brain Sciences, 12(10), 1281. https://doi.org/10.3390/brainsci12101281
Harding, I. H., Solowij, N., Harrison, B. J., Takagi, M., Lorenzetti, V., Lubman, D. I., Seal, M. L., Pantelis, C., & Yücel, M. (2012). Functional connectivity in brain networks underlying cognitive control in chronic cannabis users. Neuropsychopharmacology, 37(7), 1923–1933. https://doi.org/10.1038/npp.2012.39
Hillard, C. J. (2015). The Endocannabinoid Signaling System in the CNS: A Primer. International review of neurobiology, 125, 1–47. https://doi.org/10.1016/bs.irn.2015.10.001
Hindocha, C., Freeman, T. P., Schafer, G., Gardener, C., Das, R. K., Morgan, C. J., & Curran, H. V. (2015). Acute effects of delta-9-tetrahydrocannabinol, cannabidiol and their combination on facial emotion recognition: a randomised, double-blind, placebo-controlled study in cannabis users. European neuropsychopharmacology : the journal of the European College of Neuropsychopharmacology, 25(3), 325–334. https://doi.org/10.1016/j.euroneuro.2014.11.014
Hirvonen, J., Goodwin, R. S., Li, C.-T., Terry, G. E., Zoghbi, S. S., Morse, C., Pike, V. W., Volkow, N. D., Huestis, M. A., & Innis, R. B. (2012). Reversible and regionally selective downregulation of brain cannabinoid CB1 receptors in chronic daily cannabis smokers. Molecular Psychiatry, 17, 642–649. https://doi.org/10.1038/mp.2011.82
Hughes, J. R., Fingar, J. R., Budney, A. J., Naud, S., Helzer, J. E., & Callas, P. W. (2014). Marijuana use and intoxication among daily users: an intensive longitudinal study. Addictive behaviors, 39(10), 1464–1470. https://doi.org/10.1016/j.addbeh.2014.05.024
Hutter, C. M. (n.d.). Genome-wide association studies (GWAS). National Human Genome Research Institute. Genome.gov. Retrieved April 30, 2025, from https://www.genome.gov/genetics-glossary/Genome-Wide-Association-Studies-GWAS
Jang, S.-K., Saunders, G., Liu, M., Jiang, Y., Liu, D. J., & Vrieze, S. (2022). Genetic correlation, pleiotropy, and causal associations between substance use and psychiatric disorder. Psychological Medicine, 52(5), 968–978. https://doi.org/10.1017/S003329172000272X
Johnson E. C., Hatoum A. S., Deak J. D., Polimanti R., Murray R. M., Edenberg H. J., Gelernter J., Di Forti M., and Agrawal A. (2021) The relationship between cannabis and schizophrenia: a genetically informed perspective. Addiction, 116: 3227–3234. https://doi.org/10.1111/add.15534
Johnson, E. C., Austin-Zimmerman, I., Thorpe, H. H. A., Levey, D. F., Baranger, D. A. A., Colbert, S. M. C., Demontis, D., Khokhar, J. Y., Davis, L. K., Edenberg, H. J., Di Forti, M., Sanchez-Roige, S., Gelernter, J., & Agrawal, A. (2024). Cross-ancestry genetic investigation of schizophrenia, cannabis use disorder, and tobacco smoking. Neuropsychopharmacology, 49, 1655–1665. https://doi.org/10.1038/s41386-024-01886-3
Karniol, I. G., Shirakawa, I., Kasinski, N., Pfeferman, A., & Carlini, E. A. (1974). Cannabidiol interferes with the effects of delta 9 - tetrahydrocannabinol in man. European journal of pharmacology, 28(1), 172–177. https://doi.org/10.1016/0014-2999(74)90129-0
Karschner, E. L., Darwin, W. D., McMahon, R. P., Liu, F., Wright, S., Goodwin, R. S., & Huestis, M. A. (2011). Subjective and physiological effects after controlled Sativex and oral THC administration. Clinical pharmacology and therapeutics, 89(3), 400–407. https://doi.org/10.1038/clpt.2010.318
Kearn, C. S., Greenberg, M. J., DiCamelli, R., Kurzawa, K., & Hillard, C. J. (1999). Relationships between ligand affinities for the cerebellar cannabinoid receptor CB1 and the induction of GDP/GTP exchange. Journal of neurochemistry, 72(6), 2379–2387. https://doi.org/10.1046/j.1471-4159.1999.0722379.x
Kraemer, M., Madea, B., & Hess, C. (2019). Detectability of various cannabinoids in plasma samples of cannabis users: Indicators of recent cannabis use? Drug Testing and Analysis, 11(10), 1498–1506. https://doi.org/10.1002/dta.2682
Kuepper, R., Ceccarini, J., Lataster, J., van Os, J., van Kroonenburgh, M., van Gerven, J. M. A., Marcelis, M., Van Laere, K., & Henquet, C. (2013). Delta-9-tetrahydrocannabinol-induced dopamine release as a function of psychosis risk: 18F-fallypride positron emission tomography study. PLOS ONE, 8(7), e70378. https://doi.org/10.1371/journal.pone.0070378
Lawn, W., Trinci, K., Mokrysz, C., Borissova, A., Ofori, S., Petrilli, K., Bloomfield, M., Haniff, Z. R., Hall, D., Fernandez-Vinson, N., Wang, S., Englund, A., Chesney, E., Wall, M. B., Freeman, T. P., & Curran, H. V. (2023). The acute effects of cannabis with and without cannabidiol in adults and adolescents: A randomised, double-blind, placebo-controlled, crossover experiment. Addiction, 118(7), 1282–1294. https://doi.org/10.1111/add.16154
Levine, A., Clemenza, K., Rynn, M., & Lieberman, J. (2017). Evidence for the risks and consequences of adolescent cannabis exposure. Journal of the American Academy of Child & Adolescent Psychiatry, 56(3), 214–225. https://doi.org/10.1016/j.jaac.2016.12.014
Lorenzetti, V., Kowalczyk, M., Duehlmeyer, L., Greenwood, L. M., Chye, Y., Yücel, M., Whittle, S., & Roberts, C. A. (2023). Brain Anatomical Alterations in Young Cannabis Users: Is it All Hype? A Meta-Analysis of Structural Neuroimaging Studies. Cannabis and cannabinoid research, 8(1), 184–196. https://doi.org/10.1089/can.2021.0099
Lucas, C. J., Galettis, P., & Schneider, J. (2018). The pharmacokinetics and the pharmacodynamics of cannabinoids. British Journal of Clinical Pharmacology, 84(11), 2477–2482. https://doi.org/10.1111/bcp.13710
Lutz, B. (2020). Neurobiology of cannabinoid receptor signaling . Dialogues in clinical neuroscience, 22(3), 207–222. https://doi.org/10.31887/DCNS.2020.22.3/blutz
Matochik, J. A., Eldreth, D. A., Cadet, J.-L., & Bolla, K. I. (2005). Altered brain tissue composition in heavy marijuana users. Drug and Alcohol Dependence, 77(1), 23-30. https://doi.org/10.1016/j.drugalcdep.2004.06.011
Mayo Clinic Laboratories. (n.d.). Marijuana. Retrieved February 15, 2025, from https://news.mayocliniclabs.com/therapeutics/drug-class-testing/marijuana/
Mayo, L. M., Asratian, A., Lindé, J., Holm, L., Nätt, D., Augier, G., Stensson, N., Vecchiarelli, H. A., Balsevich, G., Aukema, R. J., Ghafouri, B., Spagnolo, P. A., Lee, F. S., Hill, M. N., & Heilig, M. (2020). Protective effects of elevated anandamide on stress and fear-related behaviors: Translational evidence from humans and mice. Molecular Psychiatry, 25, 993–1005. https://doi.org/10.1038/s41380-018-0215-1
McCarthy, J. (2023, August 10). Fully half of Americans have tried marijuana. Gallup. https://news.gallup.com/poll/509399/fully-half-americans-tried-marijuana.aspx
Meyer, H., Lee, F., & Gee, D. (2018). The role of the endocannabinoid system and genetic variation in adolescent brain development. Neuropsychopharmacology, 43, 21–33. https://doi.org/10.1038/npp.2017.143
Miller, M. L., Chadwick, B., Dickstein, D. L., Purushothaman, I., Egervari, G., Rahman, T., Tessereau, C., Hof, P. R., Roussos, P., Shen, L., Baxter, M. G., & Hurd, Y. L. (2019). Adolescent exposure to Δ⁹-tetrahydrocannabinol alters the transcriptional trajectory and dendritic architecture of prefrontal pyramidal neurons. Molecular Psychiatry, 24(4), 588–600. https://doi.org/10.1038/s41380-018-0243-x
Mørland, J., & Bramness, J. G. (2020). Δ9-tetrahydrocannabinol (THC) is present in the body between smoking sessions in occasional non-daily cannabis users. Forensic Science International, 309, 110188. https://doi.org/10.1016/j.forsciint.2020.110188
Myran, D. T., Harrison, L. D., Pugliese, M., Solmi, M., Anderson, K. K., Fiedorowicz, J. G., Perlman, C. M., Webber, C., Finkelstein, Y., & Tanuseputro, P. (2023). Transition to schizophrenia spectrum disorder following emergency department visits due to substance use with and without psychosis. JAMA Psychiatry, 80(11), 1169–1174. https://doi.org/10.1001/jamapsychiatry.2023.3582
Myran, D. T., Pugliese, M., Harrison, L. D., Solmi, M., Anderson, K. K., Fiedorowicz, J. G., Finkelstein, Y., Manuel, D., Taljaard, M., Webber, C., & Tanuseputro, P. (2025a). Changes in incident schizophrenia diagnoses associated with cannabis use disorder after cannabis legalization. JAMA Network Open, 8(2), e2457868. https://doi.org/10.1001/jamanetworkopen.2024.57868
Myran, D. T., Pugliese, M., McDonald, A. J., Xiao, J., Fischer, B., Finkelstein, Y., Tanuseputro, P., Firth, J., Pakpour, A., Hsu, C.-W., Chang, W.-C., & Solmi, M. (2025b). Cannabis use disorder emergency department visits and hospitalizations and 5-year mortality. JAMA Network Open, 8(2), e2457852. https://doi.org/10.1001/jamanetworkopen.2024.57852
Owens, M. M., Sweet, L. H., & MacKillop, J. (2021). Recent cannabis use is associated with smaller hippocampus volume: High-resolution segmentation of structural subfields in a large non-clinical sample. Addiction Biology, 26(1), e12874. https://doi.org/10.1111/adb.12874
Papariello, A., Taylor, D., Soderstrom, K., & Litwa, K. (2021). CB1 antagonism increases excitatory synaptogenesis in a cortical spheroid model of fetal brain development. Scientific Reports, 11, 9356. https://doi.org/10.1038/s41598-021-88750-2
Pasman, J. A., Verweij, K. J. H., Gerring, Z., Stringer, S., Sanchez-Roige, S., Treur, J. L., Abdellaoui, A., Nivard, M. G., Baselmans, B. M. L., Ong, J.-S., Ip, H. F., van der Zee, M. D., Bartels, M., Day, F. R., Fontanillas, P., Elson, S. L., 23andMe Research Team, de Wit, H., Davis, L. K., MacKillop, J., ... Vink, J. M. (2018). GWAS of lifetime cannabis use reveals new risk loci, genetic overlap with psychiatric traits, and a causal effect of schizophrenia liability. Nature Neuroscience, 21(8), 1161–1170. https://doi.org/10.1038/s41593-018-0206-1
Patel, S., & Hillard, C. J. (2009). Role of endocannabinoid signaling in anxiety and depression. In D. Kendall & S. Alexander (Eds.), Behavioral neurobiology of the endocannabinoid system (Vol. 1, pp. 347–371). Springer. https://doi.org/10.1007/978-3-540-88955-7_14
Patrick, M. E., Miech, R. A., Johnston, L. D., & O’Malley, P. M. (2024). Monitoring the Future Panel Study annual report: National data on substance use among adults ages 19 to 65, 1976–2023. Institute for Social Research, University of Michigan. https://monitoringthefuture.org/wp-content/uploads/2024/07/mtfpanel2024.pdf
Pauselli, L. (2018). Chapter 8 - Cannabis-induced psychotic disorders. In M. T. Compton & M. W. Manseau (Eds.), The complex connection between cannabis and schizophrenia (pp. 183–197). Academic Press. https://doi.org/10.1016/B978-0-12-804791-0.00008-2
Puder, D. (Host). (2019, May 1). Marijuana and Mental Health (No. 44) [Audio podcast episode]. In Psychiatry & Psychotherapy Podcast. Emotion Connection. https://www.psychiatrypodcast.com/psychiatry-psychotherapy-podcast/2019/5/1/marijuana-and-mental-health?rq=marijuana
Puder, D. (Host). (2019, Oct. 23). Does Cannabis Use Increase Schizophrenia and Psychosis? (No. 64) [Audio podcast episode]. In Psychiatry & Psychotherapy Podcast. Emotion Connection. https://www.psychiatrypodcast.com/psychiatry-psychotherapy-podcast/2019/10/17/does-cannabis-increase-schizophrenia-and-psychosis-thc?rq=marijuana
Puder, D. (Host). (2020, Sept. 17).The Big Five: Neuroticism Part 1 (No. 92) [Audio podcast episode]. In Psychiatry & Psychotherapy Podcast. Emotion Connection. https://www.psychiatrypodcast.com/psychiatry-psychotherapy-podcast/strongepisode-092-strongthe-big-five-neuroticism-part-1
Puder, D. (Host). (2024, January 19). Adverse Childhood Experiences and Their Lasting Impact on Health: A Comprehensive Guide (No. 203) [Audio podcast episode]. In Psychiatry & Psychotherapy Podcast. Emotion Connection. https://www.psychiatrypodcast.com/psychiatry-psychotherapy-podcast/episode-203-adverse-childhood-experiences-and-their-lasting-impact-on-health-a-comprehensive-guide?rq=203
Puder, D. (Host). (2024, February 2). Adverse Childhood Experiences Part 2: Measurement, Impact on Future Mental Health, Dissociation, and Timing of Trauma (No. 204) [Audio podcast episode]. In Psychiatry & Psychotherapy Podcast. Emotion Connection. https://www.psychiatrypodcast.com/psychiatry-psychotherapy-podcast/episode-204-adverse-childhood-experiences-part-2-measurement-impact-on-future-mental-health-dissociation-and-timing-of-trauma?rq=204
Puder, D. (Host). (2024, July 19). Adverse Childhood Experiences - HPA axis & Brain changes: cortisol, amygdala, hippocampus, cytokines, & epigenetics (Part 3 of ACE series) (No. 217) [Audio podcast episode]. In Psychiatry & Psychotherapy Podcast. Emotion Connection. https://www.psychiatrypodcast.com/psychiatry-psychotherapy-podcast/episode-217-adverse-childhood-experiences-part-3-aces?rq=217
Puder, D. (Host). (2025, March 28). Clozapine & Schizophrenia with Michael Cummings, MD (No. 236) [Audio podcast episode]. In Psychiatry & Psychotherapy Podcast. Emotion Connection. https://www.psychiatrypodcast.com/psychiatry-psychotherapy-podcast/episode-236-clozapine-schizophrenia-treatment-michael-cummings
Rault, O., Romeo, B., Butlen-Ducuing, F., Rari, E., Benyamina, A., & Martelli, C. (2022). Impact of cannabis use and its cessation on the dosage and the efficacy of antipsychotic drugs in in- and outpatients with schizophrenia taking medication: A systematic review and meta-analysis. Journal of Psychiatric Research, 156, 713–721. https://doi.org/10.1016/j.jpsychires.2022.11.012
Renard, J., Szkudlarek, H. J., Kramar, C. P., Jobson, C. E. L., Moura, K., Rushlow, W. J., & Laviolette, S. R. (2017). Adolescent THC Exposure Causes Enduring Prefrontal Cortical Disruption of GABAergic Inhibition and Dysregulation of Sub-Cortical Dopamine Function. Scientific reports, 7(1), 11420. https://doi.org/10.1038/s41598-017-11645-8
Richter, M., Murtaza, N., Scharrenberg, R., White, S. H., Johanns, O., Walker, S., Yuen, R. K. C., Schwanke, B., Bedürftig, B., Henis, M., Scharf, S., Kraus, V., Dörk, R., Hellmann, J., Lindenmaier, Z., Ellegood, J., Hartung, H., Kwan, V., Sedlacik, J., … Calderon de Anda, F. (2019). Altered TAOK2 activity causes autism-related neurodevelopmental and cognitive abnormalities through RhoA signaling. Molecular Psychiatry, 24(9), 1329–1350. https://doi.org/10.1038/s41380-018-0025-0
Robinson, T., Ali, M. U., Easterbrook, B., Hall, W., Jutras-Aswad, D., & Fischer, B. (2023). Risk-thresholds for the association between frequency of cannabis use and the development of psychosis: a systematic review and meta-analysis. Psychological medicine, 53(9), 3858–3868. https://doi.org/10.1017/S0033291722000502
Rossi, G., & Beck, M. (2020). A little dab will do: a case of cannabis-induced psychosis. Cureus, 12(9). https://pmc.ncbi.nlm.nih.gov/articles/PMC7544610/
Ryan, S. A., Ammerman, S. D., O’Connor, M. E., Gonzalez, L., Patrick, S. W., Quigley, J., Walker, L. R., Meek, J. Y., Johnston, M., Stellwagen, L., Thomas, J., Ware, J., & the Committee on Substance Use and Prevention, & Section on Breastfeeding. (2018). Marijuana use during pregnancy and breastfeeding: Implications for neonatal and childhood outcomes. Pediatrics, 142(3), e20181889. https://doi.org/10.1542/peds.2018-1889
Sabe, M., Zhao, N., & Kaiser, S. (2020). Cannabis, nicotine and the negative symptoms of schizophrenia: Systematic review and meta-analysis of observational studies. Neuroscience and biobehavioral reviews, 116, 415–425. https://doi.org/10.1016/j.neubiorev.2020.07.007
Scheffler, F., Phahladira, L., Luckhoff, H., du Plessis, S., Asmal, L., Kilian, S., Di Forti, M., Murray, R., & Emsley, R. (2021). Cannabis use and clinical outcome in people with first-episode schizophrenia spectrum disorders over 24 months of treatment. Psychiatry Research, 302, 114022. https://doi.org/10.1016/j.psychres.2021.114022
Schoeler, T., Ferris, J., & Winstock, A. R. (2022). Rates and correlates of cannabis-associated psychotic symptoms in over 230,000 people who use cannabis. Translational Psychiatry, 12, 369. https://doi.org/10.1038/s41398-022-02112-8
Schoeler, T., Baldwin, J. R., Martin, E., Barkhuizen, W., & Pingault, J.-B. (2024). Assessing rates and predictors of cannabis-associated psychotic symptoms across observational, experimental, and medical research. Nature Mental Health, 2, 865–876. https://doi.org/10.1038/s44220-024-00261-x
Sherif, M., Radhakrishnan, R., D’Souza, D. C., & Ranganathan, M. (2016). Human laboratory studies on cannabinoids and psychosis. Biological Psychiatry, 79(7), 526–538. https://doi.org/10.1016/j.biopsych.2016.01.011
Shimonovich, M., Pearce, A., Thomson, H., Keyes, K., & Katikireddi, S. V. (2021). Assessing causality in epidemiology: Revisiting Bradford Hill to incorporate developments in causal thinking. European Journal of Epidemiology, 36, 873–887. https://doi.org/10.1007/s10654-020-00703-7
Siebers, M., Biedermann, S. V., Bindila, L., Lutz, B., & Fuss, J. (2021). Exercise-induced euphoria and anxiolysis do not depend on endogenous opioids in humans. Psychoneuroendocrinology, 126, 105173. https://doi.org/10.1016/j.psyneuen.2021.105173
Smid, M. C., Metz, T. D., McMillin, G. A., Mele, L., Casey, B. M., Reddy, U. M., Wapner, R. J., Thorp, J. M., Saade, G. R., Tita, A. T. N., Miller, E. S., Rouse, D. J., Sibai, B., Costantine, M. M., Mercer, B. M., Caritis, S. N., & the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) Maternal-Fetal Medicine Units (MFMU) Network. (2022). Prenatal nicotine or cannabis exposure and offspring neurobehavioral outcomes. Obstetrics & Gynecology, 139(1), 21–30. https://doi.org/10.1097/AOG.0000000000004632
Smith, R. T., & Gruber, S. A. (2023). Contemplating cannabis? The complex relationship between cannabinoids and hepatic metabolism resulting in the potential for drug-drug interactions. Frontiers in Psychiatry, 13, 1055481. https://doi.org/10.3389/fpsyt.2022.1055481
Solowij, N., Broyd, S., Greenwood, L. M., van Hell, H., Martelozzo, D., Rueb, K., Todd, J., Liu, Z., Galettis, P., Martin, J., Murray, R., Jones, A., Michie, P. T., & Croft, R. (2019). A randomised controlled trial of vaporised Δ9-tetrahydrocannabinol and cannabidiol alone and in combination in frequent and infrequent cannabis users: acute intoxication effects. European archives of psychiatry and clinical neuroscience, 269(1), 17–35. https://doi.org/10.1007/s00406-019-00978-2
Stuyt, E. (2018). The problem with the current high potency THC marijuana from the perspective of an addiction psychiatrist. Missouri Medicine, 115(6), 482–486. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6312155/
Substance Abuse and Mental Health Services Administration (SAMHSA). (2022a). 2021 National Survey on Drug Use and Health: National maps of prevalence estimates, by state. U.S. Department of Health and Human Services. https://www.samhsa.gov/data/sites/default/files/reports/rpt39463/2021NSDUHsaeMaps110122/2021NSDUHsaeMap110122.htm#fig2e
Substance Abuse and Mental Health Services Administration (SAMHSA). (2022b). Key substance use and mental health indicators in the United States: Results from the 2021 National Survey on Drug Use and Health (HHS Publication No. PEP22-07-01-005, NSDUH Series H-57). Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. https://www.samhsa.gov/data/report/2021-nsduh-annual-national-report
van Os, J., Bak, M., Hanssen, M., Bijl, R. V., de Graaf, R., & Verdoux, H. (2002). Cannabis use and psychosis: A longitudinal population-based study. American Journal of Epidemiology, 156(4), 319–327. https://doi.org/10.1093/aje/kwf043
Vaucher, J., Keating, B. J., Lasserre, A. M., Gan, W., Lyall, D. M., Ward, J., Smith, D. J., Pell, J. P., Sattar, N., Paré, G., & Holmes, M. V. (2018). Cannabis use and risk of schizophrenia: A Mendelian randomization study. Molecular Psychiatry, 23(6), 1287–1292. https://doi.org/10.1038/mp.2016.252
Verweij, K. J. H., Abdellaoui, A., Nivard, M. G., Sainz Cort, A., Ligthart, L., Draisma, H. H. M., Minică, C. C., Gillespie, N. A., Willemsen, G., Hottenga, J.-J., Boomsma, D. I., & Vink, J. M. (2017). Erratum to “Short communication: Genetic association between schizophrenia and cannabis use” [Drug Alcohol Depend. 171 (2017) 117–121]. Drug and Alcohol Dependence, 173, e1–e2. https://doi.org/10.1016/j.drugalcdep.2017.02.001
Verweij, K. J. H., Vink, J. M., Abdellaoui, A., Gillespie, N. A., Derks, E. M., & Treur, J. L. (2022). The genetic aetiology of cannabis use: From twin models to genome-wide association studies and beyond. Translational Psychiatry, 12(1), 489. https://doi.org/10.1038/s41398-022-02215-2
Vid Prkačin, M., Banovac, I., Petanjek, Z., & Hladnik, A. (2023). Cortical interneurons in schizophrenia - cause or effect?. Croatian medical journal, 64(2), 110–122. https://doi.org/10.3325/cmj.2023.64.110
Weiland, B. J., Thayer, R. E., Depue, B. E., Sabbineni, A., Bryan, A. D., & Hutchison, K. E. (2015). Daily marijuana use is not associated with brain morphometric measures in adolescents or adults. The Journal of neuroscience : the official journal of the Society for Neuroscience, 35(4), 1505–1512. https://doi.org/10.1523/JNEUROSCI.2946-14.2015
Zammit, S., Allebeck, P., Andreasson, S., Lundberg, I., & Lewis, G. (2002). Self-reported cannabis use as a risk factor for schizophrenia in Swedish conscripts of 1969: Historical cohort study. BMJ, 325(7374), 1199. https://doi.org/10.1136/bmj.325.7374.1199
Zuardi, A. W., Teixeira, N. A., & Karniol, I. C. (1984). Pharmacological interaction of the effects of delta 9-trans-tetrahydrocannabinol and cannabidiol on serum corticosterone levels in rats. Archives internationales de pharmacodynamie et de therapie, 269(1), 12–19. https://pubmed.ncbi.nlm.nih.gov/6087750/